
The incidence of cardiovascular diseases is at a tipping point. While until recently morbidity and mortality from these diseases have continuously declined, this trend is now reversing. In order to prevent the number of sick and dying people from increasing, we need to collect data and use it as a basis for appropriate treatment and prevention. According to the President of the Czech Society for Cardiology, Aleš Linhart, randomised trials remain the gold standard in cardiology in this respect, but they also need to collect real-life data that include all possible patients, including those with comorbidities or poorer compliance. This issue was the subject of the 2nd Annual International Panel of the Permanent Conference on Healthcare.
„In cardiovascular prevention, we need to stop patting ourselves on the back and say that the reality of the last forty years is changing. We were used to cardiovascular morbidity and mortality falling, only part of that was due to the healthcare sector. The socio-economic situation was also improving, which was doubly true for the countries of Central Europe. However, data from developed countries now show that cardiovascular morbidity and mortality are increasing, and these are patients in an age group limited by an upper limit, so they are not the oldest ones, and this is not the effect of an ageing population,“ says Aleš Linhart.
The current trend in the Czech Republic is not entirely clear because the data has been distorted by the COVID-19 pandemic. This caused people to reduce their use of healthcare services, especially initially, so that 20 to 25 percent fewer heart attack patients were admitted to centres in the first months of the pandemic. These are usually patients afraid to seek medical help. Nevertheless, already before 2020, it became apparent for some cardiovascular diseases that the trend was turning in our country too and that we would follow developed countries with a slight delay.
The fact is that cardiovascular morbidity and mortality are related to the economic performance of a country. The Czech Republic is currently in a place where every economic downturn is accompanied by a relatively steep increase in the risk of cardiovascular morbidity and mortality. This was, after all, demonstrated by Irish data from 2008, the time of the economic crisis, which demonstrated that cardiovascular mortality had increased by 17 per cent.
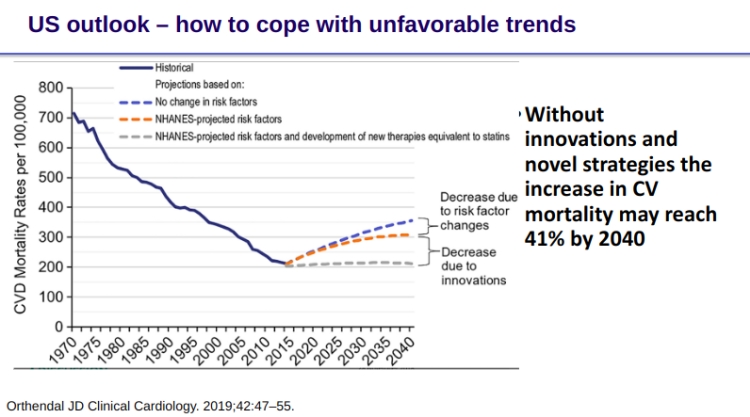
Without innovation and new strategies, mortality from cardiovascular diseases will increase.
To reverse this trend, it is therefore essential to begin taking active steps. If we do not so, cardiovascular mortality and morbidity will rise by 40 per cent by 2040, according to projections based on US figures. On the other hand, if we want to stabilise the rising curve, we need to invest in new drugs, treatment strategies, prevention, and education.
„Cardiovascular prevention is very much about individual responsibility, and if we do not have an informed population, it cannot be responsible,“ points out Aleš Linhart.
On the other hand, he said, the repeated appeals to invest in prevention are already starting to be perceived. „Knocking on the door has an effect. Various prevention programmes are being launched and we are starting to invest more in prevention. The Ministry of Health is appearing to listen that prevention is important to reverse the negative trend,“ says Professor Linhart.
We need data from different sources
However, in order to best tailor prevention and therapy, we need data. In cardiology, data from a large number of randomised clinical trials or meta-analyses are considered to be the most valuable evidence for making recommendations. These are followed by data from a single randomised trial or large non-randomised trials, and lastly by expert consensus, small studies, retrospective studies, or registers.
„We are now seeing a number of attempts to replace randomised clinical trials with real-world and post-hoc analysis of clinical data from various registers. I would like to cite that this is not a 100% sensible way to go. Randomised trials are the most valuable evidence we have, although we must be careful not to extrapolate their results beyond what happened in them. On the other hand, if we take registers and observational studies, we know that we are able to adjust for many variables, so we need to obtain not only medical data but also socioeconomic data on our patients. Even then, the adjustment may not be 100% valid,“ warns Professor Linhart.
Mohlo by vás zajímat


A session on the knowledge base for public health policymaking. From left: Prof. Herwig Ostermann, Director of the National Institute of Public Health, Austria, Tomáš Cikrt, Editor-in-Chief of Zdravotnický deník, Prof. Róbert Babeľa, State Secretary of the Slovak Ministry of Health, Prof. Reuven Zimlichman, Head of Cardiovascular Research Institute, Sackler Faculty of Medicine, Tel-Aviv University, Israel, and Prof. Aleš Linhart, President of the Czech Society for Cardiology. Photo: Stanislav Pecháček
As an example, statins demonstrated a clear effect on survival in a randomised trial, while two non-randomised trials showed no effect. Similarly, DPP-4 inhibitors used in diabetes appeared to reduce cardiovascular events by more than 60 per cent in an observational study, but this was subsequently refuted in a randomised trial.
„Randomised trials will continue to be the gold standard in cardiology and should not be replaced by analyses of registers. However, real-world data are also invaluable because they can provide data beyond randomised trials, monitor many more patients, and, most importantly, provide safety signals that relatively small randomised trials cannot. It also serves to confirm the effect,“ Linhart explains.

At the same time, even randomised trials have their pitfalls, he says. It is a relatively sterile world, where patients with typical characteristics are enrolled, who are usually cooperative and understand what doctors want them to do. But the real world is different because many patients are frail, may take doctors‘ instructions with a grain of salt or have comorbidities. This is also why we need to collect data from the real world.
„The outlook for cardiovascular diseases is quite dark if we do not share data, accumulate and interpret them properly and prepare for what is to come. My personal feeling is that we have often turned a blind eye to this so far and tried to regulate our budgets, especially the drug policy, at any cost so that we can come out next year. And we forget that if we want to save money in ten years, the investment must arrive now,“ concludes Aleš Linhart.
Michaela Koubová









